

Illustration by Karol Banach
Zion Levy remembers the excitement that he and his daughter felt while poring over body scans in 2019, watching small black dots, representing melanoma metastases, shrink away and eventually vanish. They weren’t Levy’s scans. He didn’t even know who the scans came from, but he did share a connection with them.
About five years earlier, Levy had been diagnosed with melanoma, but he was in remission thanks to a powerful immunotherapy called nivolumab. Because he had responded well to the drug, doctors at the Sheba Medical Center in Tel HaShomer, Israel, asked whether he would consider donating his stool — and the microbes inside — to possibly help others who had failed to respond or whose cancers had become resistant to treatment. He agreed to rigorous tests, blood draws and detailed questions about what he ate most (pizza). Levy made his donation, packed it into a cooler, and then called a taxi hired by the hospital. As with any transplant, travel time mattered. Doctors wanted the sample to arrive in less than 90 minutes.
Once there, Levy’s faeces were tested for pathogens, diluted, homogenized, centrifuged and sifted down to a refined microbial broth that could be freeze-dried and packed into capsules. Levy’s enthusiasm for the project convinced Ben Boursi, an oncologist at the Sheba Medical Center, who was leading the study, to share the anonymized scans of a recipient of his donated microbes. Today, that person has gone more than three years without evidence of cancer and has become a donor in a similar melanoma-treatment trial. It’s a legacy that Levy feels good about. “I am very proud that I can save lives. I would like to do it again,” he says.
The Israeli trial1 and one led by researchers in the United States2 were the first of their kind to use faecal microbial transfer (FMT) to prime patients for a better response to immunotherapies, powerful anticancer drugs that unleash the body’s own immune system against tumours. The results of these two studies, published in Science last year, were modest — of 26 people who had previously failed to respond to immunotherapy, around one in three did so after FMT — but they garnered a lot of attention.
“Even though they only had few patients, there was a cohort in each group that could overcome their resistance. I think that’s great, because it demonstrates that we’re on the right track,” says Brenda Wilson, a microbiologist at the University of Illinois at Urbana-Champaign. The next step, Wilson says, is to work out which patients will respond and which won’t.
Today, at least 30 FMT trials are under way around the world, run by academic laboratories and pharmaceutical companies, with results beginning to trickle in.
Increasingly, research is showing that the gut microbiome can have good or bad effects on the progression of distant tumours, the side effects of treatments and the ability of the immune system to pick off cancer cells. Some research has linked specific bacteria to beneficial effects, which could point to tailored treatments. And scientists are exploring the role of diet and gut-microbe diversity, as well as revealing interactions between the organisms that reside in the gut and those that live in tumours themselves, potentially opening up new targets for treatment.
Translating these observations into actual therapies, however, could prove difficult. Boursi has treated 30 people, and estimates that between 50 and 100 individuals worldwide have received FMT to supplement cancer therapy. As new studies get off the ground, researchers will need strategies for identifying the best donors, scaling up the transplant procedure and making it affordable.
Still, Boursi and others are undeterred. He says that the approach could open the door to an “era of ecological oncology”, one in which a better understanding of tumour, host, the immune system and resident microbes will lead to better treatment.
Seminal trials
Boursi’s interest started in 2006. A hiking trip while he was finishing up his medical studies left him contemplating the tumour-like growths on trees, known as burrs, that are sometimes the result of a plant’s response to an infection. He started thinking about how tumours and bacteria might interact in the human body, but colleagues dissuaded him from pursuing the idea. They told him to “focus on genetics instead”, Boursi recalls. Still, he pressed ahead with epidemiological studies that linked cancer and the microbiome, exploring how antibiotics could change cancer risk and how diet could modify gut microbes.
Ten years later, a picture started to emerge of the microbiome as a modifiable organism in both health and disease, and the link with cancer had begun to get attention. This trend coincided with an explosion of interest in immunotherapies. These drugs have had remarkable success in many types of cancer, but don’t work in every patient — only 15–20% of people have a long-lasting response.
Data supporting the influence of microbes in the success or failure of these therapies started piling up at cancer conferences and in top journals. A frequently mentioned 2015 study by Thomas Gajewski, an oncologist at the University of Chicago, Illinois, and his colleagues showed that the balance of gut microbes in mice determined whether the rodents responded to a certain type of immunotherapy3. Changing the microbiome made mice respond better. In 2018, three papers echoed those results in people with melanoma who were treated with checkpoint inhibitors — a type of immunotherapy that essentially reminds stalled immune cells to attack cancer cells4–6. The presence or absence of certain key microorganisms in the gut seemed to affect the likelihood of a response.
Soon, researchers across the world had FMT clinical trials under way. The procedure had shown some success in helping people with recurring infections of Clostridioides difficile, a bacterium that can cause a debilitating diarrhoeal disorder. Melanoma is a prime target for FMT support because it is a common cancer and only sometimes responds well to immunotherapies.
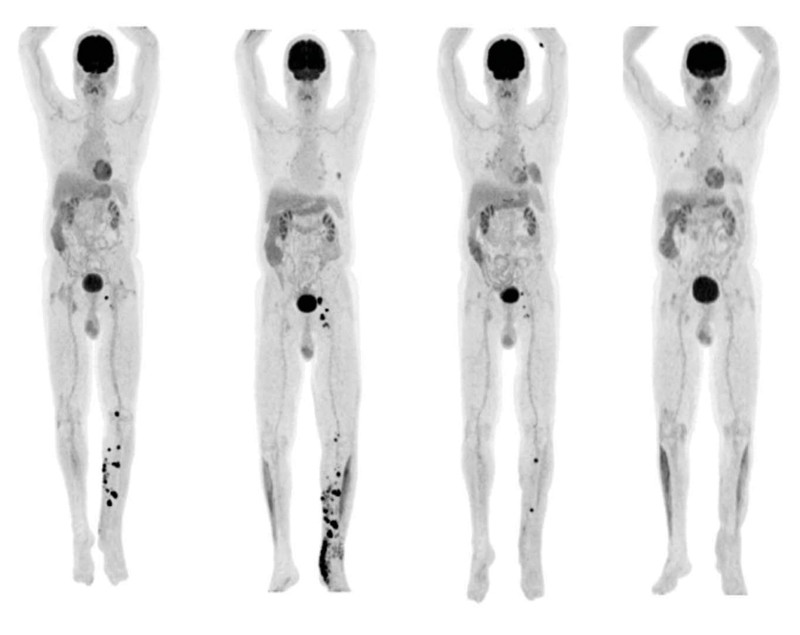
Scans from one trial participant in Israel show metastases completely resolving after treatment.Credit: E. N. Baruch et al./Science
“This is now a movement that didn’t exist before,” says Hassane Zarour, a dermatologist and cancer immunologist at the University of Pittsburgh Medical Center (UPMC) Hillman Cancer Center in Pennsylvania. “What was scepticism is now positivity.”
Zarour led the study that accompanied Boursi’s in Science last year. Together, these first clinical trials treated a total of 26 people. The Israeli study enrolled ten individuals with late-stage melanoma whose cancer had progressed despite treatment with a checkpoint inhibitor. Only three overcame resistance to the therapy, and two of these only partially; incidentally, all three responders received FMT from Levy. All of the five participants who received material from a different donor (also a cancer survivor) failed to respond.
The US trial, run by UPMC and the National Cancer Institute in Bethesda, Maryland, enrolled 16 people with metastatic melanoma whose cancer had progressed after immunotherapy. This trial used seven donors who had had a lasting response to immunotherapy for melanoma. Of the 16 recipients, 6 showed a response and 3 of these were a complete response, although there were no clear signs that stool from any one donor had a more or less positive effect.
Scientists still don’t know what it means to have “good stools” — donor material that promotes an efficient anticancer response — says David Pinato, a consulting oncologist and head of the developmental therapeutics research programme at Imperial College London. “You need to know if what you are giving is actually active locally,” he says. “You might just be giving a placebo at the end of the day.”
Different studies have conflicting findings as to which microbes are most important. Although a diverse microbiome has strongly been linked to health, Levy’s was less diverse than the other microbiome used in the Israeli study, and yet it seemed to be beneficial.
“Ultimately researchers need to come up with the secret sauce, a consortia of bugs with good functional qualities that could promote immunity and overall health,” says Jennifer Wargo, an oncologist at the MD Anderson Cancer Center in Houston, Texas, and an author of the Israeli study. But finding that optimal mix might be impossible. Microbiome composition varies greatly by ethnicity, geography and diet, says Alexander Khoruts, a gastroenterologist and medical director of the University of Minnesota’s microbiota therapeutics programme in Minneapolis.
The team behind the US trial published a parallel study in Nature Medicine in March, aiming to identify organisms associated with response and non-response, and testing whether machine learning could help to match microbiota donors and recipients7. Right now, scientists don’t know whether cancer survivors have a bad microbiome but a good immune system or the other way around, says Amiran Dzutsev, an immunologist at the National Cancer Institute and one of the study’s lead authors.
More recent work by a Canadian team used FMT from donors who have not had cancer, to test whether it can prevent resistance to immunotherapy in people who haven’t received it before. The team presented the results of their early-stage trial in June at the American Society of Clinical Oncology meeting in Chicago. Primary resistance is the biggest problem facing the field, says Saman Maleki, an immunologist at Western University in London, Canada, and team leader for the trial. The Canada-wide study enrolled 20 people with advanced melanoma. After FMT and immunotherapy, 3 people showed a complete response, 13 a partial response and 3 showed stable disease (one participant died of melanoma).
The data are preliminary8, but Maleki is pleased with the results so far. “We have seen not only a good safety signal from all these studies but also early signals hinting at the ability of microbiome-based treatments to improve efficacy of immunotherapy.”
Zeynep Eroglu, an oncologist at the Moffitt Cancer Center in Tampa, Florida, points out that the response rate in this study was only a little higher than for immunotherapy alone. Typically around 40% of late-stage melanomas show some response to immunotherapy. But, she says, “I do commend the investigators for an attempt to move this into the first-line setting in treatment of metastatic melanoma”. She adds that convincing people to try FMT before immunotherapy might not be easy. “It will be interesting with these studies to see where they go.”
Manipulating a complex ecosystem
Identifying the ideal stool for donation might not be a matter of which microbes it holds, but rather what they do, says Wargo. Looking at the metabolites bacteria produce is crucial to characterizing treatments, says Khoruts. That might in turn alter how they are delivered.
Another issue to consider is the microbiome of the tumour itself. Microbes make up about 25% of the tumour environment and their presence can promote or block antitumour immunity. In the past few years, work by Ravid Straussman, a cancer biologist at the Weizmann Institute of Science in Rehovot, Israel, has shown that microbes in tumours can mediate resistance to chemotherapy9. Straussman’s team has also identified specific bacteria located inside tumour cells10.
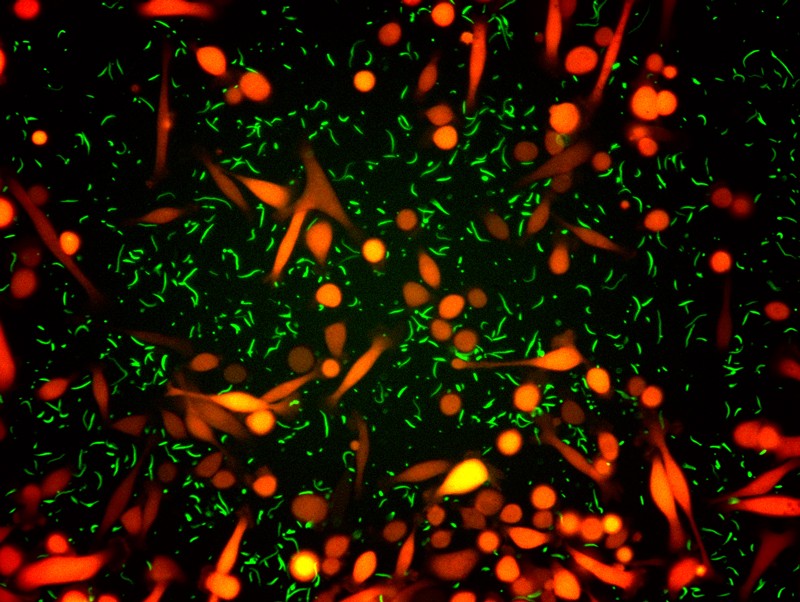
Cancer cells (orange) co-cultured with bacteria (green): many tumours have their own microbiome, which might interact with microbes in other parts of the body.Credit: Straussman Lab/Weizmann Institute of Science
Microbes travel to tumours from many areas — including the gut, the oral cavity and the bloodstream — depending on the cancer, says Boursi. “We think there are different origins,” says Florencia McAllister, an oncologist at the MD Anderson Cancer Center. “We know this from comparing, within the same patient, the tumour with adjacent tissue and with gut and oral microbiomes.” Researchers are now starting to eavesdrop on the crosstalk between tumour microbes and gut microbes to find out whether and how they influence one another.
Some studies are starting to unpick the complexities. A 2019 Cell paper studied people with pancreatic adenocarcinoma — a diagnosis with a generally poor survival rate — from two geographically distinct areas, Baltimore and Houston11. Long-term responders — people who survived five years or more — had a more diverse tumour microbiome than did those who survived less than five years. Some of the microbes in the tumour, it seems, were derived from the gut. FMT from the long-term survivors delayed tumour growth in mice with pancreatic cancer and boosted their immune cells.
The team now has a clinical trial to test those ideas in people with pancreatic cancer. “First, we want to see if the transplanted microbiota is stable and can be maintained over time,” says McAllister, who is lead author on the Cell paper. In the long term, the study will analyse whether altering the gut microbes with FMT will directly change microbes in the tumour.
But also unresolved is the extent to which diet will affect microbiota transplants, which is probably the least studied area of this effort. Khoruts says the question most commonly asked by people who receive FMT for C. difficile infections is what they should eat after the procedure. He tells them to minimize processed foods and emphasize a plant-based diet, because beneficial gut microbes like complex carbohydrates.
Epidemiological studies around the world show that diet influences gut-microbiome profiles even more so than do people’s genes, says Christine Spencer, director of informatics at the Parker Institute for Cancer Immunotherapy in San Francisco, California. Spencer is the lead author of a 2021 study showing that people with melanoma who ate high-fibre diets were more likely to respond favourably to immunotherapy, whereas over-the counter probiotics were associated with worse outcomes12.
Easing toxic side effects
After Amnon Shany was diagnosed with malignant melanoma in 2017, he volunteered for a clinical trial testing the immune checkpoint inhibitor, pembrolizumab, an antibody that inactivates a protein that cancer cells use to hide from immune cells. Almost immediately, side effects took hold; arthritis limited all movement and he had to quit playing tennis. In the course of two years, dehydration from severe diarrhoea sent him to the hospital six times. The metastases shrank but didn’t disappear.
“It wasn’t a nice time,” says Shany, an oral surgeon in Ness Ziona, Israel. But, he adds, “I didn’t think for a moment that I had another choice. This was reality.”
Then, a year and a half ago, his physician called about trying FMT with another round of immunotherapy. Shany’s first response was shock. “If I went through all this agony, the last thing on Earth that I have in mind is to swallow faeces of somebody else,” he says.
But he didn’t hesitate for long. He signed the consent form and joined the trial, during the chaos of the COVID-19 pandemic. He had one course of FMT through colonoscopy, a procedure he’d come to dread. That was followed up with two more doses of 32 capsules — the size of olives — which he had to swallow in one setting. Shany nicknamed them “zeppelins”. Then he went back on the immunotherapy. This time, it seemed to work better. His last PET scan, in May, was clean.
Shany’s FMT came from the lone, full responder in the first Israeli clinical trial, making Shany, essentially, a second-generation recipient of Levy’s donation. Not only did the immunotherapy work, but its side effects were minimized, much to Shany’s relief.
That’s a big hope for researchers, that microbiota modulation might ease the severe side effects immunotherapy can bring. FMT is being tested in pilot studies at Memorial Sloan Kettering Cancer Center in New York City, the University of Minnesota Medical School and elsewhere in patients undergoing stem-cell transplants, to offset damage to the microbiome from cycles of chemotherapy, radiotherapy and antibiotics.
“Major causes of non-cancer mortality in this setting are infections and graft-versus-host disease,” says Khoruts.
Scaling up
But should microbiota transplants for cancer go mainstream, they could strain the limited supply of donors. Few of the people who want to donate actually qualify. Maleki screens 40 people to get one suitable donor. They need to be tested for bacterial and viral infections — the COVID-19 pandemic caused some studies to halt until appropriate tests could be developed.
And although stool preparation is straightforward, the need to prevent cross-contamination means researchers can process just one donor sample in a room per day. Even the most efficient academic facilities will probably not be able to handle expanded demand, says Khoruts. Microbiota transplants might have to be taken over by a commercial or non-profit enterprise. “Doing it on a large scale requires capital investment,” says Khoruts. There are already signs of this materializing, with some clinical trials being run by companies.
In the end, FMT for cancer might end up being a convergence of several technologies, says Zarour, using either human-derived or engineered bacteria to create drugs. This effort requires a greater understanding of the complexity of microbial communities in cancer than researchers have now.
And as technologies emerge, they might be priced in a way that not everyone can afford, says Colleen Kelly, a gastroenterologist at Brown University in Providence, Rhode Island. There are already disparities in access to cancer treatment. Kelly has found13 that Black and Hispanic people are less likely to receive FMT for C. difficile infections than are white people. She is looking into whether these disparities are due to lack of health-care access, referrals or cost. Kelly worries that the same thing will happen with FMT given as part of cancer treatment, for which she expects new therapeutics to be expensive. Even with the uncertainties, trials are moving forwards and expanding to other cancers. Such trials, says Boursi, “will change the way we see cancer, the way we investigate cancer, and will eventually change the way we treat cancer”.
More News
I study artefacts left in prehistoric caves
How artificial intelligence is helping to identify global inequalities
Tackling ‘wicked’ problems calls for engineers with social responsibility