
For Rick Doblin, 2023 could be a landmark year: the year that the US government decides whether it will allow the use of hallucinogenic drugs to treat mental illness.
Doblin, who is based in Belmont, Massachusetts, is the founder and president of the non-profit organization Multidisciplinary Association for Psychedelic Studies (MAPS). He has spent nearly 40 years researching whether the experience produced by the psychedelic drug MDMA — also called ecstasy or molly — can help people with post-traumatic stress disorder (PTSD). In 2021, MAPS’s phase III clinical trial of 90 people with PTSD found that those who received MDMA coupled with psychotherapy were twice as likely to recover from the condition as were those who received psychotherapy with a placebo1 (see ‘Response to MDMA therapy’).
Source: Ref. 1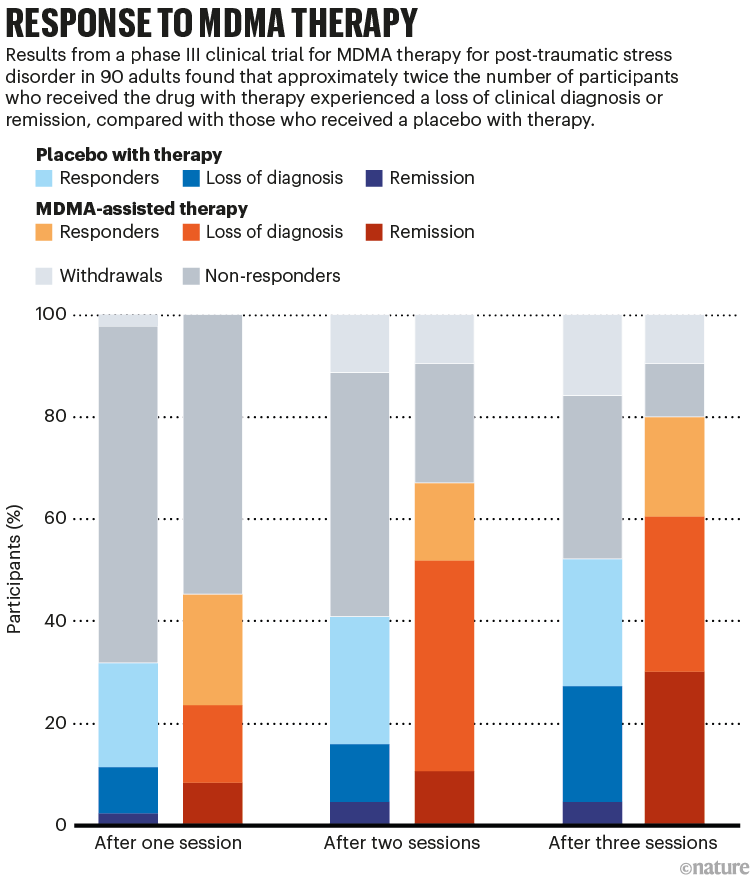
MAPS has now completed a second, larger trial that it says has also produced positive results. After that study is published in the coming months, MAPS plans to ask the US Food and Drug Administration (FDA) to approve the drug as a legal treatment for PTSD, probably by October. FDA approval would mark a turning point for psychedelic drugs, which have long been illegal and thus difficult to study. With MAPS nearing the finish line, Doblin is optimistic that things will go smoothly. “I don’t think there’ll be tricky questions or anything, the results are great,” he says.
This shift towards taking psychedelic therapy seriously is happening outside the United States as well. In February, Australia approved MDMA as a treatment for PTSD, although the drug will remain highly restricted. Doblin and others hope that the changing attitudes will open the door for other therapeutic psychedelics, including ketamine, ayahuasca, LSD (acid), psilocybin (the active ingredient in magic mushrooms) and many synthetic chemicals currently in development. One analysis has projected that the psychedelics market could be worth more than US$8 billion by 2028.
But many questions remain in the short term, chiefly how MDMA will be administered and by whom. MAPS officials say that the drug must be given in concert with a psychotherapy protocol developed by the company’s scientists, but the FDA does not typically regulate such treatments. And it’s unclear whether approving MDMA on the basis of MAPS’s data would ease the way for other companies hoping to study and develop the drug, or whether anyone would even want to. MDMA has been around since 1912 and cannot be patented, creating little financial incentive. And if problems arise after the drug is approved, researchers worry that political and public sentiment could turn against psychedelics, setting the whole field back.
But Doblin still envisions treatment centres sprouting up around the world — he predicts that more than 6,000 will emerge in the United States alone — where people with PTSD and other psychiatric illnesses can safely and legally use MDMA and other psychedelics under the guidance of therapists. Beyond this, he hopes ultimately for full legalization that would allow anyone to take the drugs however they wish. “MAPS has been the beacon to kind of take on this work,” says neuroscientist Amy Kruse, who is chief investment officer at venture capital firm Satori Neuro and is based in Annapolis, Maryland. “There are many people that can benefit from this treatment, and I think it shows a pathway for the potential rescheduling of other molecules.”
A regulatory puzzle
Doblin, who has spoken openly about his own experiences taking psychedelic drugs, founded MAPS in 1986, a year after the US government banned MDMA. The goal was to revive research that had begun in the 1960s, which suggested that MDMA and LSD could treat a number of psychiatric conditions, including PTSD. The theory holds that MDMA allows people to confront their trauma by dampening the fight-or-flight response much in the way alcohol does, but without the confusion and forgetfulness. Whereas many PTSD therapies direct a person to concentrate on a traumatizing event — potentially retraumatizing them in the process — MDMA elevates positive emotions and allows people to make connections that might not have otherwise seemed obvious, according to proponents. Therapists had administered it to thousands of patients before the ban, only some of them under the auspices of clinical trials.

Chronic pain can be treated — so why are millions still suffering?
After the drug was outlawed, psychiatrists remained sceptical about its efficacy for decades. Still, the twentieth-century data allowed MAPS to skip early safety trials and immediately begin phase II trials to assess MDMA’s efficacy as a PTSD treatment in half a dozen countries.
The intense experiences that come with taking MDMA created a unique problem for regulators. The FDA typically requires at least two double-blind, placebo-controlled studies. But there has typically been little doubt among participants and therapists about who is receiving the drug.
Without a true placebo control, a trial of a psychiatric drug will almost certainly produce positive results, says Erick Turner, a psychiatrist at Oregon Health & Science University in Portland, who has served on FDA advisory committees. “Patients know what they’re getting and believe in it,” he says. “They’re going to be biased by that knowledge.”
Doblin anticipated this issue — and, in 2017, the FDA approved a ‘special protocol’ for MAPS. After the treatment sessions, each participant’s symptoms were evaluated by psychologists who did not administer the drug and did not know who was in each group. With this protocol in place, the FDA has agreed to base its decisions on the reported efficacy and not take issue with the study design. Outside advisers to the FDA can still raise concerns, however.
Doblin worries what the regulators will do about the psychotherapy component. In trials, the drug is administered by a pair of MAPS-trained therapists who guide the participant’s experience through scripted sessions that also allow for improvisation. The FDA does not regulate the guided-therapy component, only the drug — but Doblin says that the two are inseparable. “What we believe is that the results that we got were not from MDMA,” Doblin says. “They were from highly trained therapists who are then using MDMA.”
A MAPS spokesperson says that the organization expects that the drug’s prescribing label will state that MDMA needs to be administered in combination with therapy. The FDA has done this previously with some other psychiatric drugs, including naltrexone. Because the FDA does not oversee behavioural-health interventions, the spokesperson adds, insurers or government payers are likely to enforce this requirement.
MAPS is also sponsoring trials of different types of psychological co-treatment, including cognitive therapies and group therapy, to see whether these are better or more efficient.
Rick Doblin, president of the Multidisciplinary Association for Psychedelic Studies.Credit: Tony Luong/New York Times/Redux/eyevine
The unscripted component of the guided therapy also concerns Turner, because it introduces another variable that could influence efficacy. “The psychotherapy is a moving target, and changes depending upon the patient’s response,” he says. A person who gets the placebo would have a therapy experience very different from that of someone who gets MDMA. An FDA spokesperson says the agency is “generally unable to discuss existing or potential applications”.
Safety problems, not necessarily with the drug itself, are also a concern. A woman enrolled in MAPS’s phase II study reported that she had been assaulted by her therapists; videos show them lying in bed with her and kissing her during a 2015 MDMA session. One of the therapists later started a sexual relationship with her, and she eventually reported him to the police and sued him in civil court. In his response, the therapist said that the relationship was consensual. The case was settled out of court.

How ecstasy and psilocybin are shaking up psychiatry
MAPS fired the therapists and updated its consent forms to inform participants that such behaviour could happen but is not permissible. Doblin says that puts the burden on the therapist. “It’s a general problem, it happens with or without MDMA,” he says. In surveys, a small percentage of therapists admit to having been sexually involved with clients during or after therapy, despite the ethical guidelines of psychology associations2.
There are strong signs that the government is leaning towards approval. In 2022, The Intercept published a letter from an official at the US Department of Health and Human Services saying that it anticipated that the FDA would approve MDMA by 2024. And in 2017, the FDA granted ‘breakthrough’ status to both MDMA and psilocybin, putting the drugs on a regulatory fast track to approval.
Organizations such as the American Psychological Association (APA) have been cautiously optimistic: a 2022 statement said that, although current scientific evidence is inadequate for the use of psychedelics outside clinical trials, “APA supports continued research and therapeutic discovery into psychedelic agents.” Still, the organization has warned that treatments should be approved by regulators instead of “by ballot initiatives or popular opinion”.
Racing to approval
Some worry that premature approval of the drugs could frustrate scientific progress. In 2020, the state of Oregon voted to legalize psilocybin for therapeutic use. And in February, researchers around the world were shocked when Australia’s Therapeutic Goods Administration announced that it would legalize MDMA as a PTSD treatment as of 1 July. The administration has not yet provided details on what kind of training will be required to administer the drug. So far, only one person has been treated with MDMA as part of an Australian study, and he dropped out of the trial. “We don’t have anything to indicate this is safe and effective,” says Stephen Bright, a psychologist at Edith Cowan University in Perth, Australia, who is running the MDMA trial and is currently recruiting more participants. He worries that the reclassification could halt trials because no one would want to end up in a placebo group.
Even Doblin was taken aback by Australia’s decision. “I’m nervous about what’s going on and about the level of training that will be required,” he says. MAPS is planning to train several dozen Australian practitioners later this year, but Doblin worries that other training programmes will be insufficient.
Australia’s move could put pressure on the FDA to approve MDMA and open a larger market in the United States. But Mason Marks, a law professor at Florida State University in Tallahassee who studies drug policy, isn’t convinced that approving MAPS’s application will open the door for other psychedelic drugs or providers, at least not any time soon. In 2018, the agency approved an epilepsy drug called Epidiolex, which is developed from a non-psychoactive component of cannabis. But all other medical cannabis formulations remain federally illegal. Marks suspects that the agency will similarly approve MAPS’s protocol and specific MDMA capsule formulation, rather than reclassifying the drug and effectively making it legal.
Psychedelics move from agents of rebellion towards therapeutics
Such a move would essentially leave MAPS as the only source of legal MDMA treatment outside clinical trials, which Marks worries could hamper innovation. “It does create an asymmetry between MAPS and other groups that might want to do research that could help us understand the safety,” he says.
Kruse thinks that FDA approval would nevertheless foster innovation. “The PTSD landscape is quite broad, and I don’t think this is a winner-take-all environment,” she says. If MAPS is the only one allowed to develop MDMA and administer treatment, she says, it could incentivize other companies to develop and patent similar, alternative chemicals.
MAPS intends to commercialize MDMA for profit, but its long-term plans are unclear. In 2014, the organization created a public-benefit corporation (PBC) — a company that attempts to balance shareholders’ financial interests and the public interest. A spokesperson for MAPS PBC declined to answer whether it plans to patent its formulation, or to speculate on future plans. “We think we will be the first to bring MDMA-assisted therapy to patients,” the spokesperson says, which should mean that MAPS can market the formulation exclusively for five and a half years.
Beyond that, Doblin says, MAPS PBC hasn’t decided what its future will look like. The company says that its therapist training programme has made millions of dollars from therapists, medical practices and donors paying to train practitioners in the clinical trials. But if MDMA therapy is integrated into standard psychiatry and psychology training programmes, which is Doblin’s goal, that revenue stream could dry up. He would also like to see MDMA fully legalized, which would make it more difficult to sell for profit. “I’m on the knife’s edge between capitalism and altruism,” Doblin says.
Regardless of MAPS’s financial future, he is cheering for researchers developing other psychedelic drugs, such as psilocybin, or repurposing MDMA as a treatment for depression and traumatic brain injury. Even if the FDA approval takes longer than anticipated, he says, the groundwork has been laid.
“The endgame is mass mental health,” he says. “But it will take several generations.”
More News
Publisher Correction: High carrier mobility along the [111] orientation in Cu2O photoelectrodes – Nature
Mapping genotypes to chromatin accessibility profiles in single cells – Nature
Alphafold 3.0: the AI protein predictor gets an upgrade